Speech audiometry
Authors: Benjamin Chaix, Rebecca Lewis
Contributors: Diane Lazard, Sam Irving
Speech audiometry is routinely carried out in the clinic. It is complementary to pure tone audiometry, which only gives an indication of absolute perceptual thresholds of tonal sounds (peripheral function), whereas speech audiometry determines speech intelligibility and discrimination (between phonemes). It is of major importance during hearing aid fitting and for diagnosis of certain retrocochlear pathologies (tumour of the auditory nerve, auditory neuropathy, etc.) and tests both peripheral and central systems.
Speech audiogram
The speech recognition threshold (SRT) is the lowest level at which a person can identify a sound from a closed set list of disyllabic words.
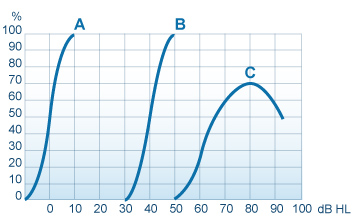
The word recognition score (WRS) testrequires a list of single syllable words unknown to the patient to be presented at the speech recognition threshold + 30 dBHL. The number of correct words is scored out of the number of presented words to give the WRS. A score of 85-100% correct is considered normal when pure tone thresholds are normal (A), but it is common for WRS to decrease with increasing sensorineural hearing loss.
The curve ‘B’, on the other hand, indicates hypoacusis (a slight hearing impairment), and ‘C’ indicates a profound loss of speech intelligibility with distortion occurring at intensities greater than 80 dB HL.
It is important to distinguish between WRS, which gives an indication of speech comprehension, and SRT, which is the ability to distinguish phonemes.
Phonetic materials and testing conditions
Fonix audiometric test monosyllabic words:
List n°1A :
Laud
Boat
Pool
Nag
Limb
Shout
Sub
Vine
Dime
Goose
Greyhound
Schoolboy
Inkwell
Whitewash
Pancake
Mousetrap
Eardrum
Headlight
Birthday
Duck pond
Fonix audiometric test: disyllabic words
List n°2A :
Pick
Room
Nice
Said
Fail
South
White
Keep
Dead
Loaf
Mousetrap
Eardrum
Headlight
Birthday
Duck pond
The test stimuli can be presented through headphones to test each ear separately, or in freefield in a sound attenuated booth to allow binaural hearing to be tested with and without hearing aids or cochlear implants. Test material is adapted to the individual’s age and language ability.
What you need to remember
In the case of a conductive hearing loss:
- the response curve has a normal ‘S’ shape, there is no deformation
- there is a shift to the right compared to the reference (normal threshold)
- there is an increase in the threshold of intelligibility
In the case of sensorineural hearing loss:
- there is an increased intelligibility threshold
- the curve can appear normal except in the higher intensity regions, where deformations indicate distortions
Phonetic testing is also carried out routinely in the clinic (especially in the case of rehabilitation after cochlear implantation). It is relatively long to carry out, but enables the evaluation of the real social and linguistic handicaps experienced by hearing impaired individuals. Cochlear deficits are tested using the “CNC (Consonant Nucleus Consonant) Test” (short words requiring little mental recruitment – errors are apparent on each phoneme and not over the complete word) and central deficits are tested with speech in noise tests, such as the “HINT (Hearing In Noise Test)” or “QuickSIN (Quick Speech In Noise)” tests, which are sentences carried out in noise.
Speech audiometry generally confirms pure tone audiometry results, and provides insight to the perceptual abilities of the individual. The intelligibility threshold is generally equivalent to the average of the intensity of frequencies 500, 1000 and 2000 Hz, determined by tonal audiometry (conversational frequencies). In the case of mismatch between the results of these tests, the diagnostic test used, equipment calibration or the reliability of the responses should be called into question.
Finally, remember that speech audiometry is a more sensitive indicator than pure tone audiometry in many cases, including rehabilitation after cochlear implantation.